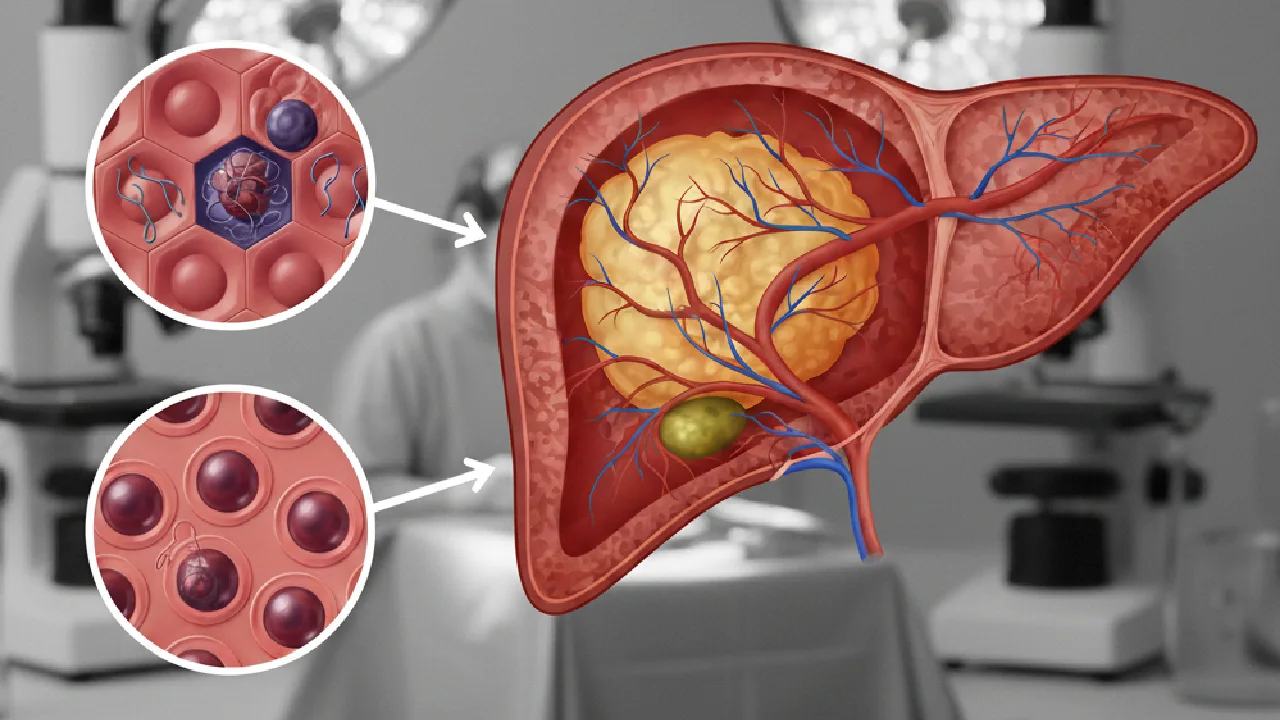
What Are Liver Metastases?
Liver metastases are the most common malignant liver tumours, far outnumbering primary liver cancer (hepatocellular carcinoma). They occur when cancer cells spread from a primary tumour to the liver via the bloodstream or lymphatics. The most common primary sources are colorectal (50% of patients develop liver metastases), breast, lung, gastric and pancreatic cancers.
Symptoms
Small liver metastases are often asymptomatic and detected on surveillance imaging. Larger deposits may cause: right upper quadrant pain or heaviness, jaundice (if biliary compression), ascites, nausea and loss of appetite, weight loss, or signs of liver dysfunction in advanced disease.
Diagnosis
CT scan (triphasic): Most widely used for detection and characterisation. Liver MRI: More sensitive for small or indeterminate lesions. Superior for pre-surgical planning. PET-CT: Assesses overall disease extent. Tumour markers: CEA for colorectal, CA 19-9 for pancreatic/biliary, AFP for hepatocellular. Biopsy: May be required for diagnosis when primary is unknown.
Treatment of Colorectal Liver Metastases
Surgical resection: The only potentially curative treatment. 5-year survival of 30–50% in resected patients. Two-stage hepatectomy or ALPPS allow resection when the future liver remnant is inadequate. Ablative techniques: Radiofrequency ablation (RFA), microwave ablation for small, surgically inaccessible lesions. Chemotherapy: FOLFOX, FOLFIRI ± targeted agents as neoadjuvant or palliative. SIRT/TACE: Intra-arterial therapies for unresectable hepatic disease.
Conversion Surgery
Initially unresectable liver metastases may become resectable after response to systemic chemotherapy. This "conversion" strategy has expanded the pool of patients who can benefit from curative surgery.
Have you been diagnosed with liver metastases? At Quenet Torrent Institute our hepatobiliary surgical oncology team evaluates resectability and plans optimal treatment strategies. Request a consultation.